
Key highlights
- Nearly one-third of children under five in India are stunted
- Among Scheduled Caste (SC) children, those living south of the Vindhyas are ~0.24 standard deviations taller and 7-8 percentage points less likely to be stunted than those in the north.
- No comparable north–south difference exists for upper-caste children, indicating that these disparities are not purely geographic or economic, but rooted in social exclusion and caste-based discrimination
Child malnutrition remains one of the most pressing challenges in India. Nearly one-third of children under the age of five are stunted: a condition reflecting chronic undernutrition that has lasting consequences for physical growth, cognitive development, and later-life outcomes.
But these outcomes are not evenly distributed. A closer look reveals stark inequalities across social groups. In earlier work , we show that children from historically marginalized caste groups are significantly more likely to be stunted than their more advantaged counterparts. These gaps are large, persistent, and visible across the country.
What explains these gaps? A substantial body of research has pointed to factors such as poverty, sanitation, birth order, and gender bias. These are undoubtedly important. Yet, taken together, they do not fully account for the scale of the disparities we observe across caste groups.
In recent work published in the Journal of Economic Behavior & Organization, we take a step further and ask whether caste-based discrimination may be an important part of the story.
A simple comparison across a historical boundary
To examine this, we make use of a historical and social divide within India: the Vindhyas mountain range. The Vindhyas have long marked a boundary between the regions where the areas to the North of the Vindhyas range comprise the North Central and Central plains, also known as the Indo-Gangetic plain, once home to the Indus Valley Civilization around 3000 BCE, and later known as “Aryavarta” during the Vedic period (c. 1500–600 BCE). This is what was historically the historical geographical span of Hinduism, bounded to the south by the Vindhyas mountain range (Thapar, 1990; Sharma, 2016).
Drawing on this history, we suggest that the caste system and practices such as untouchability more strongly define the social code of the caste system to the North of the Vindhyas range compared to the South of the Vindhyas range. This variation provides a useful lens. If discrimination plays a role in shaping child health, we might expect outcomes for marginalized groups to differ across this boundary in ways that are not observed for more advantaged groups.
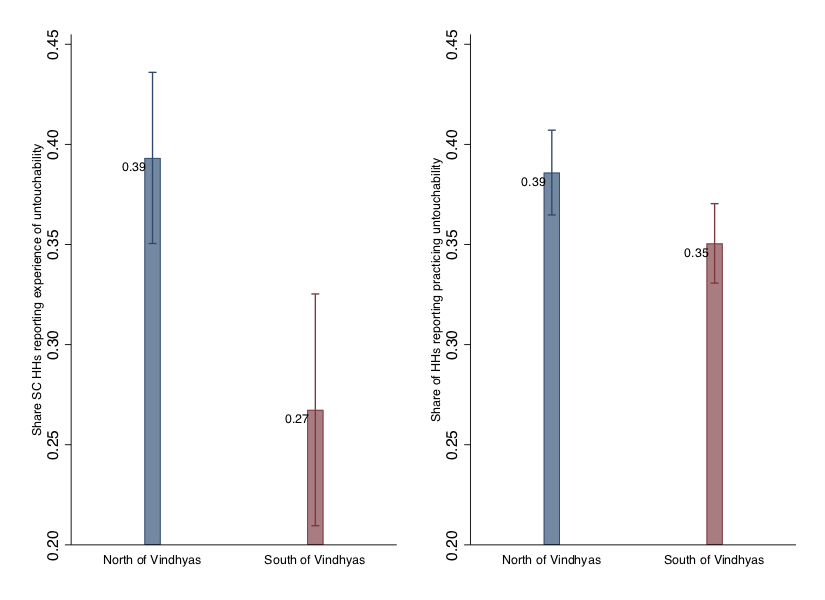
Figure 1 above shows a striking pattern. Focusing on districts within a narrow band—100 kilometers on either side of the Vindhyas—we find clear differences in the prevalence and experience of untouchability. Households to the north report substantially higher experience of these untouchability than those to the south.
What we see in the data
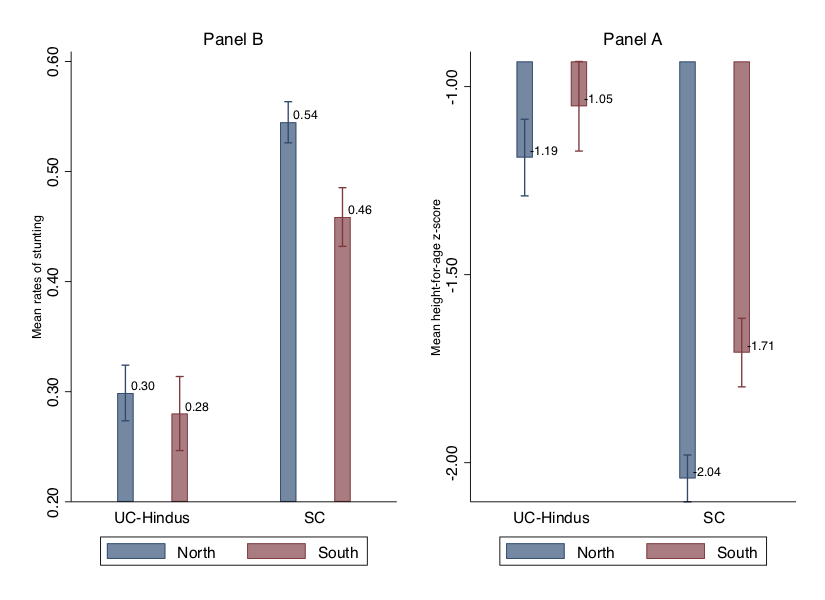
We begin with a simple comparison. Figure 2 below plots stunting rates and height-for-age scores for children living within 100km to the north and south of the Vindhyas. The contrast is revealing.
For children from Hindu upper-caste groups, there is little to no difference in stunting rates or height outcomes across the boundary. In other words, living north or south of the Vindhyas does not appear to matter for this group.
For children from the Scheduled Castes (SCs), however, the picture is very different. Those living to the south of the Vindhyas have substantially better outcomes—lower stunting rates and higher height-for-age scores—than those living to the north.
When we formalize this comparison using a statistical (difference-in-differences) framework, the differences remain large. SC children living south of the Vindhyas are, on average, about 0.24 standard deviations taller and roughly 7 to 8 percentage points less likely to be stunted than their counterparts to the north. Given a baseline stunting rate of around 29 percent, this represents a sizable improvement.
Could it be something else?
Of course, differences across regions could reflect many factors. We therefore conduct a series of checks to rule out alternative explanations. First, we show that the results are robust to different ways of defining the comparison area—expanding the geographic window or excluding areas very close to the boundary. The patterns remain stable.
Next, we examine whether the results could be driven by economic or socioeconomic differences. Household wealth, as expected, is strongly associated with child health outcomes overall—children from wealthier households are less likely to be stunted. However, what matters for our analysis is not the level of outcomes, but how they differ across the north and south of the Vindhyas. Here, we find no evidence that wealth explains the pattern we observe. In particular, poorer households do not experience any additional improvement from living south of the Vindhyas. In other words, while wealth matters in general, it does not account for the north–south differences in outcomes.
We then turn to other disadvantaged groups. If the observed pattern simply reflected broader socioeconomic disadvantage, we should expect to see similar improvements for all such groups. However, this is not what we find. For groups that are economically disadvantaged but not historically subject to caste-based discrimination—such as Scheduled Tribes (STs) or higher ranked Muslims—we do not observe comparable differences across the boundary. By contrast, the pattern is present for groups with a history of caste-based exclusion, such as the lowest rung of Muslims, who are described as Dalit Muslims. This suggests that the observed differences are not driven by disadvantage alone, but are more closely linked to the legacy of caste-based discrimination.
We also conduct placebo exercises, shifting the boundary arbitrarily northward or southward. These comparisons yield no meaningful differences, suggesting that the patterns we observe are specific to the historical divide marked by the Vindhyas.
Taken together, these results make it less likely that the observed differences are driven by general regional or economic factors.
What about underlying mechanisms?
We also explore a wide range of factors that are known to influence child health—maternal education and health, household conditions, sanitation, access to water, and broader community characteristics.
These variables matter. Accounting for them reduces the overall gap in outcomes between caste groups, highlighting the importance of material conditions and public health infrastructure.
However, a key finding remains: these factors do little to explain the difference we observe across the Vindhyas for SC children. The improvement in outcomes for those living to the south persists even after accounting for these variables.
A suggestive conclusion
Taken together, the evidence points to a consistent pattern: differences in child health outcomes across this historical boundary are concentrated among groups historically exposed to caste-based discrimination and are not easily explained by observable economic or environmental factors.
This does not allow us to make a definitive causal claim. But it is consistent with the idea that caste-based discrimination may play an important role in shaping early childhood outcomes.
If so, this has important implications. Efforts to reduce child malnutrition often focus—rightly—on improving income, nutrition, and public health infrastructure. But our findings suggest that addressing deeply embedded social norms and exclusionary practices may also be critical. Understanding and tackling these underlying social barriers could be an important step toward reducing persistent inequalities in child health in India.
To cite this analysis: Ashwini Deshpande & Rajesh Ramachandran (2026), “Discriminatory Social Norms and Early Childhood Development” Centre for Economic Data and Analysis (CEDA), Ashoka University. Published on ceda.ashoka.edu.in

